

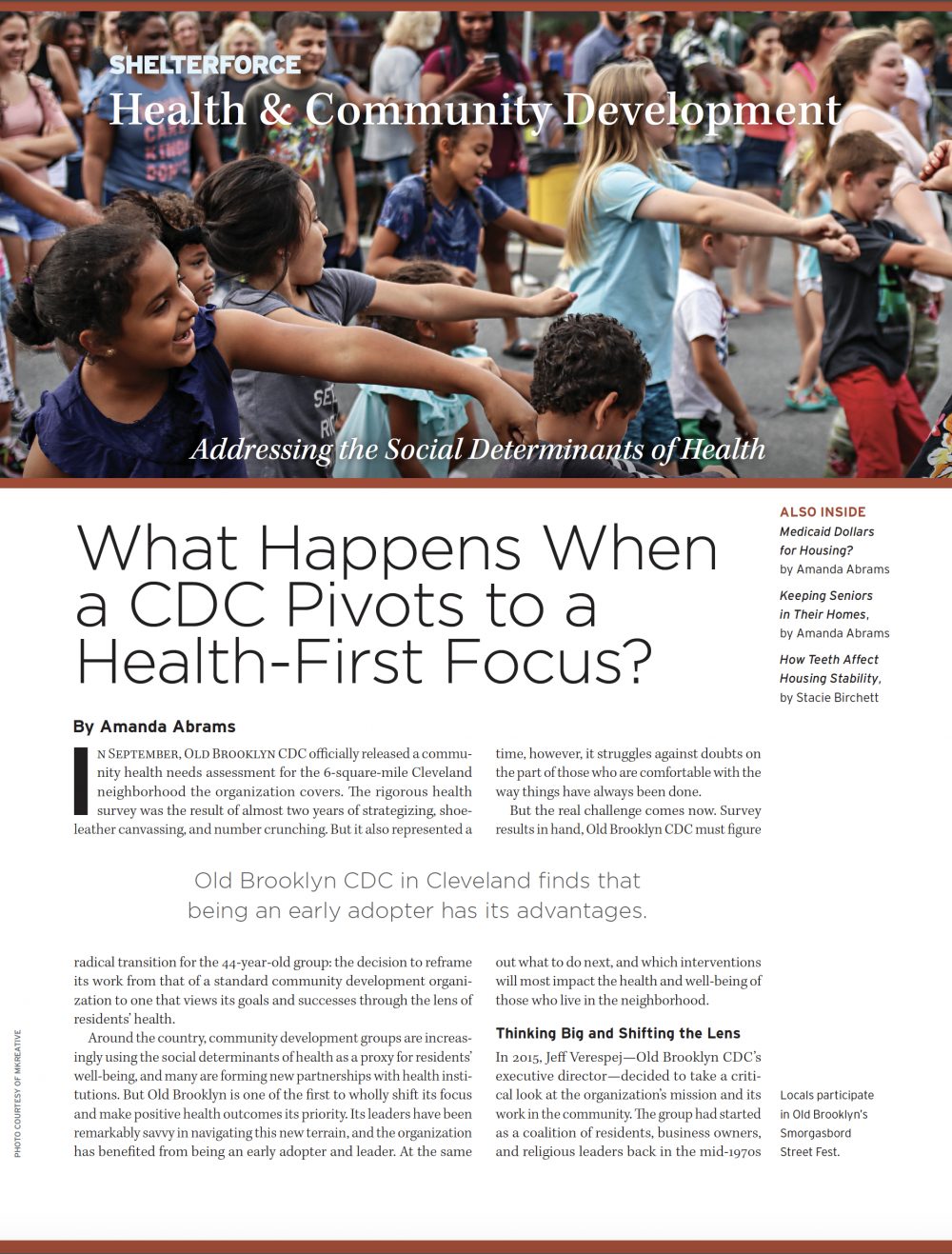
Locals participate in Old Brooklyn’s Smorgasbord Street Fest. Photo courtesy of mKreative
In September, Old Brooklyn Community Development Corporation officially released a community health needs assessment for the 6-square-mile Cleveland neighborhood the organization covers. The rigorous health survey was the result of almost two years of strategizing, shoe-leather canvassing, and number crunching. But it also represented a radical transition for the 44-year-old group: the decision to reframe its work from that of a standard community development organization to one that views its goals and successes through the lens of residents’ health.
Around the country, community development groups are increasingly using the social determinants of health as a proxy for residents’ well-being, and many are forming new partnerships with health institutions. But Old Brooklyn CDC is one of the first to wholly shift its focus and make positive health outcomes its priority. Its leaders have been remarkably savvy in navigating this new terrain, and the organization has benefited from being an early adopter and leader. At the same time, however, it struggles against doubts on the part of those who are comfortable with the way things have always been done.
But the real challenge comes now. Survey results in hand, Old Brooklyn CDC must figure out what to do next, and which interventions will most impact the health and well-being of those who live in the neighborhood.
Thinking Big and Shifting the Lens to Health
In 2015, Jeff Verespej—Old Brooklyn CDC’s executive director—decided to take a critical look at the organization’s mission and its work in the community. The group had started as a coalition of residents, business owners, and religious leaders back in the mid-1970s and largely focused on business support and housing development. But Cleveland’s largest neighborhood was changing. African American and Latinx populations were growing and the poverty rate was rising, but the community was also stratifying, with the proportion of household incomes over $100,000 increasing.
“We felt we needed a change to reflect those evolving times,” says Verespej, who had been hired a couple of years earlier. “So we took a critical look at the status quo: was it acceptable, or did we need to change?” The organization was open to thinking big.
After almost nine months of conversations with community members, stakeholders, and staff, it was the facilitator hired to help with the strategic planning process who introduced the idea of focusing on health to Verespej. “The consultant sat me down in the conference room one day and said, ‘I think you’ll be investing in community health. You’re already doing it: you’re in housing and economic opportunity, you’ve just never tied it together to be health,’” recalls Verespej.
He quickly saw the consultant’s point and jumped on the idea with enthusiasm. “What it’s about is quality of life,” says Verespej. Issues such as the safety of neighborhood streets and the distance of grocery stores selling healthy food mattered to local residents, and they fell under the organization’s existing mission: to improve the neighborhood by uniting residents and businesses. The bottom line was the same; only the health terminology would be different. “We’ve never framed it that way, that’s the shift.
“As a neighborhood that’s in between strength and instability, investing in community health as a quality-of-life strategy is critical. We don’t want to go off the edge either way and we believe that this [focus] will help as it uses data, partners, and root causes,” says Verespej.
Katie Grace Deane, associate director of research, evaluation, and field development at the Center for Community Investment, which focuses on the nexus of community development and health, says Old Brooklyn CDC may well be a leader in the community development field. “I haven’t heard of anyone refocusing the entirety of their work on health,” she says. And as long as the organization’s actions truly reflect the needs and desires of the community, she adds, it could wind up being very successful.
While unsure of what it meant for them, senior staff liked the idea; some of their titles changed, but no one left. Board members, too, were largely supportive. Still, says Verespej, “It was a multiyear process to get them to adopt the [new] strategic plan. They asked all the critical questions along the way.”
Lawyer Sean McGrane was perhaps the most skeptical board member. “When you define health very broadly, as we have, I have a concern that it’ll subsume the traditional functions of a CDC,” says McGrane. For example, Old Brooklyn CDC had long been engaged in housing rehabilitation in the area. “Is the physical infrastructure part of health?” McGrane asks rhetorically. “We had a staff member focused on education, helping with schools—is that part of health?” (The organization’s education and rehab programs have both continued.)
And there was grumbling when the organization lost funding for its code enforcement manager while simultaneously raising money for the health-oriented initiative. But by and large, board members were willing to take a “wait and see” position.
Community Health: Thirty-eight Questions
Verespej has consistently been described by colleagues and funders as ambitious, persistent, and far-sighted. Once he’d been converted to a health focus, he moved very deliberately, careful to build partnerships and alliances every step of the way. After the organization’s new strategic plan was adopted in 2016, he contacted people all over the region who were even tangentially related to the field of community health to hear their thoughts.
It was through those conversations that he and board members came up with their next steps: hiring a health fellow who would form an advisory committee and conduct a community health needs assessment (CHNA); that way, the organization could get a data-driven sense of the area’s problems before designing any programs.
To support the initiative, Verespej returned to several local funders who had provided money for the original strategic planning process to ask them to back the fruits of that process. He was largely successful. Colleen Gilson, vice president of CDC advancement for Cleveland Neighborhood Progress, an umbrella agency for the city’s CDCs, was immediately intrigued with Old Brooklyn CDC’s new ideas.
“It was unique, different, and something we thought we could certainly learn from,” says Gilson. There was risk involved, certainly, but she was impressed with Verespej’s leadership, vision, and big plans, and felt that the city’s CDCs would benefit from observing his group’s efforts to shift to a health focus—characteristics that other funders noted as well.
Her organization wound up naming Old Brooklyn CDC as one of its strategic investment grantees and awarded it a total of $300,000 of unrestricted operating dollars over three years. Two other local groups, the Cleveland Foundation and Enterprise Community Partners, committed to providing roughly $50,000 each over two years.
Funding in hand, Old Brooklyn CDC conducted a national job search for its health fellow and in May 2017, the organization hired Jennifer King, who had recently earned a doctorate in public health. Her job description was clear: “Convening a community health advisory committee, conducting a community health needs assessment, and really figuring out how to empower the residents of the neighborhood to understand what health is and how to take an active role in improving it,” says King.
Many of the stakeholders Verespej had originally spoken with became members of the advisory committee. In particular, the MetroHealth System, Cleveland’s safety net hospital that has a branch within Old Brooklyn, was engaged from very early on. Others included representatives of the city and county health departments, as well as the Better Health Partnership—a group of stakeholders focused on improving health outcomes—and the Cleveland Clinic, a local medical center with an international reputation.
After initial discussions with neighborhood residents to gain a sense of their priorities and concerns, advisory group members hammered out a set of questions for the survey. Dave Margolius, a MetroHealth doctor, Old Brooklyn CDC board member, and advisory committee member, remembers one meeting when Merle Gordon—Cleveland’s director of public health and a fellow advisory committee member—was particularly insightful.
“She came up with a great idea of asking, ‘Where do people go grocery shopping?’” he says. Answers to that question would allow the organization to pinpoint exactly how far residents have to go for groceries, and could even open the door to eventually lobbying specific stores to stock healthier items, for example.
In the end, the CHNA had 38 questions on topics like safety, green space, food accessibility, housing, child health, and substance abuse. Calling it a CHNA—the same name used by health care institutions for the audits the IRS requires, and by local and state health departments—was intentional, says Verespej: the survey was the same kind of tool used by big hospitals, simply tailored to a much smaller area. And that’s unusual. “As far as I know, this is the only one that’s been done by community-based organization for its neighborhood,” says Verespej. He and his staff hope hospitals will learn from the organization’s community-driven, bottom-up approach.
Before releasing it to the community, Old Brooklyn CDC took the extra step of getting the survey approved by the Institutional Review Board (IRB) at nearby Baldwin Wallace University. IRB approval is standard for academic research; it gives the assessment the stamp of scholarly legitimacy and enables its outcome to potentially be published in an academic journal.
Finally, in early 2018, the organization posted the survey on its social media channels, and staff members hit the streets, using whatever opportunities they could think of to reach a range of neighborhood populations. “That included going to the public library, the neighborhood recreation center, barbershops, parent-teacher night at local schools,” says King. She and other staff members quickly realized they were oversampling older white women, so they redoubled their efforts to connect with other demographics. In the end, over the course of three months, 412 people responded to the survey.
In the summer of 2018, when staff finally examined the survey’s results, there were surprises. Almost 20 percent of respondents worry about running out of food, with the same percentage reporting that they frequently have to choose between food and housing; over one-third said they spend more than 30 percent of their income on housing. Ten percent said they abuse prescription drugs, and virtually none have plans to quit doing so.
Those results show the benefits of having conducted a statistically sound survey. “It allows others who don’t necessarily have a public health background or are really involved in this work to see that [these issues] are very real,” says King.
Developing Interventions and Finding Funding
Old Brooklyn CDC held a two-day summit in September to publicly release the survey’s results and convene community developers for a conversation about health programming prompted by the survey. The event had another objective as well: to help the organization identify potential new allies. After all, “the starter’s gun has just gone off,” as Verespej puts it. With the assessment complete, it was now time to get to work identifying possible interventions to address the neighborhood’s needs.
To assist with that process, the CDC hired a community health coordinator to develop a residents’ advisory group, in order to ensure that whatever comes next is truly grassroots-driven. Jennifer King left her job for academia; the next person who fills the health fellow role will have to be action-oriented. And the organization was recently granted $80,000 by the CareSource Foundation to begin developing community health interventions.
What those interventions will look like is still murky, though. There are some ideas floating around: MetroHealth has an office of opioid safety and recently bought a drug recovery facility in the neighborhood, for example, so the organization could find a way to work with the health care group. Or Old Brooklyn CDC might work with the Greater Cleveland Food Bank to deliver food to the community’s many seniors. Or it could partner with the local farmers’ market to hold fitness events and healthy-cooking demonstrations.
But first, staff will have to figure out the organization’s identity in these activities. The strategic plan dictates that Old Brooklyn CDC act as a community backbone, but what that means is context-dependent and not always obvious. “One of the things I’ve challenged Jeff and the organization with is, ‘Let’s understand the role we play: are we a facilitator? Coordinator? Starting new services?’” says Dave Martin, the organization’s board chair. “Let’s not try to do it all. Let’s pick the next few things we think we can do effectively and gain some momentum that way.”
Indeed, Old Brooklyn CDC is already part of one new initiative. Together with MetroHealth, the organization purchased the last non-institutionally owned property near the MetroHealth branch in the neighborhood, and the two groups won a $65,000 study grant from the regional transportation agency. The plan is to turn the property into a green space—something the survey illustrated was lacking in the center of the neighborhood—and enhance its attractiveness to pedestrians.
Unsurprisingly, partnering with MetroHealth in this way is a smart and strategic decision on Old Brooklyn CDC’s part. It’s a low-cost, feel-good project, and MetroHealth is perhaps the organization’s most obvious ally. As a public hospital, its mission closely aligns with that of the CDC, but because it’s a large institution, many of the public health activities it supports can be done more nimbly and with more community support by an organization like Old Brooklyn CDC.
“Obviously, Old Brooklyn [CDC] understands way better than we can the housing market for Old Brooklyn,” says Greg Zucca, MetroHealth’s director of economic and community transformation, “or where there is lead contamination, or gaps in transportation to get people to work. Working with CDCs creates that lens.”
MetroHealth isn’t rolling in funds, though. “We’re a public health hospital; we don’t have a ton of money to be investing in a lot of things,” says Zucca. That’s largely true for other local hospitals as well, even the Cleveland Clinic; though it co-sponsored the summit in September, the nonprofit hospital posted a decline in operating revenues for the first half of 2018.
There have been challenges with other funding, too. Being an unconventional CDC isn’t always a benefit, Verespej has found. Recently he met with the community development manager of a large regional bank to talk about what Old Brooklyn CDC was doing. “We were flatly told, ‘This doesn’t fit into a community development portfolio. We love this work, but we need to see it proven before we can invest in it,’” Verespej remembers. That wasn’t the first time: not surprisingly, big institutional lenders aren’t always comfortable taking risks on new ideas.
Nor are other community development corporations fully comfortable working with Old Brooklyn CDC. Few showed up at the September summit, probably because not many have staff members explicitly tasked with community health.
Clearly, there’s a lot of work ahead for Old Brooklyn CDC. But Verespej excels at forming partnerships, and the organization—like most community development nonprofits—has become adept at leveraging funding in order to get more funding. With the CHNA as a map for its future, Old Brooklyn CDC may well find a way to greatly improve the neighborhood’s health and improve the lives of its residents.

Comments