

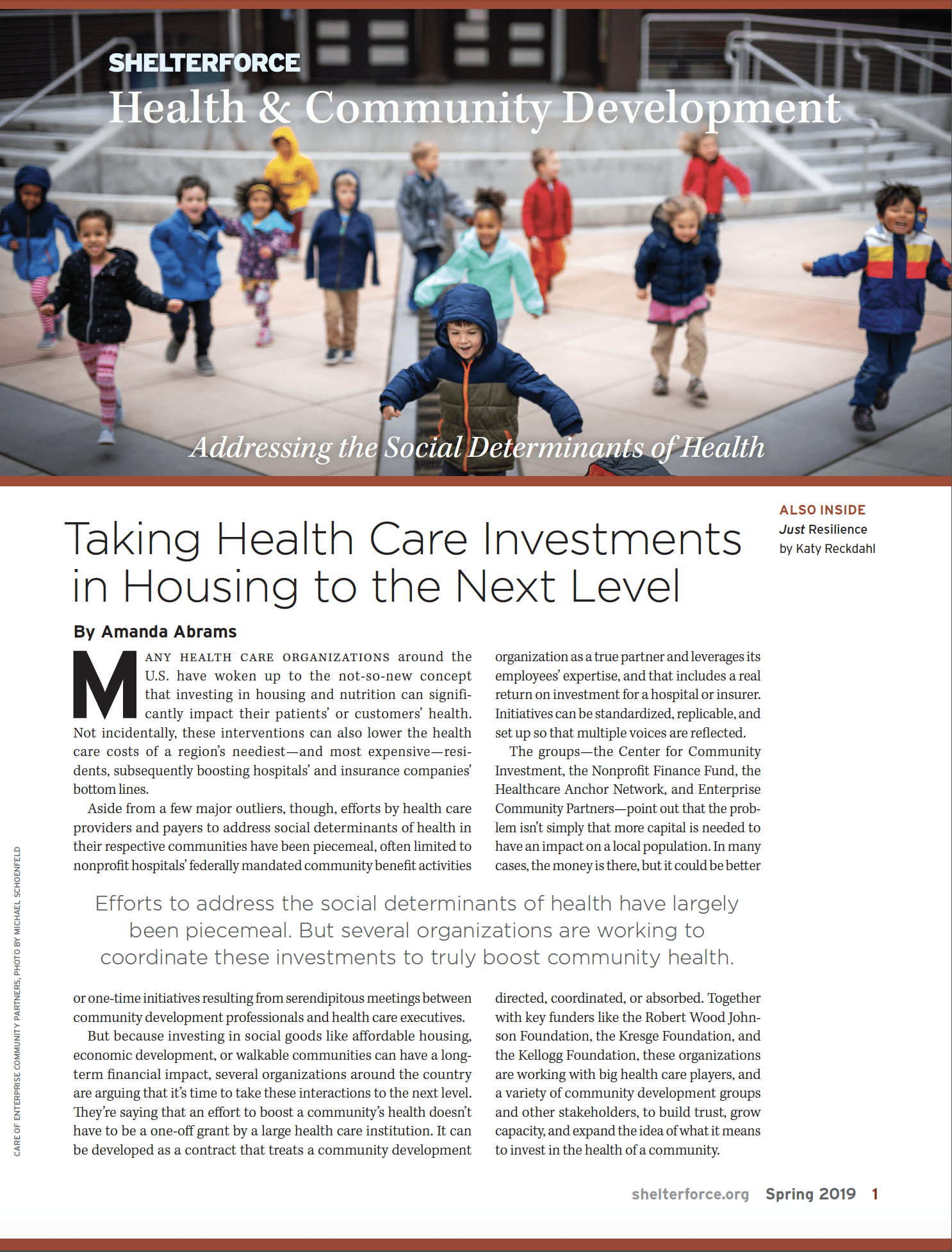
Investing in social goods like affordable housing, economic development, or walkable communities can have a long-term financial benefits. Photo by Tyrone Turner/Robert Wood Johnson Foundation
Many health care organizations around the United States have woken up to the not-so-new concept that investing in upstream factors like housing and nutrition can significantly impact their patients’ or customers’ health. Not incidentally, these interventions can also lower the health care costs of a region’s neediest—and most expensive—residents, subsequently boosting hospitals’ and insurance companies’ bottom lines.
Aside from a few major outliers, though, efforts by health care providers and payers to address social determinants of health in their respective communities have been piecemeal, often limited to nonprofit hospitals’ federally mandated community benefit activities or one-time initiatives resulting from serendipitous meetings between community development professionals and health care executives.
But because investing in social goods like affordable housing, economic development, or walkable communities can have a long-term financial impact, several organizations around the country are arguing that it’s time to take these interactions to the next level. They’re saying that an effort to boost a community’s health doesn’t have to be a one-off grant by a large health care institution. It can be developed as a contract that treats a community development organization as a true partner and leverages its employees’ expertise, and that includes a real return on investment for a hospital or insurer. Initiatives can be standardized, replicable, and set up so that multiple voices are reflected.
The groups—the Center for Community Investment, the Nonprofit Finance Fund, the Healthcare Anchor Network, and Enterprise Community Partners—point out that the problem isn’t simply that more capital is needed to have an impact on a local population. In many cases, the money is there, but it could be better directed, coordinated, or absorbed.
Together with key funders like the Robert Wood Johnson Foundation, the Kresge Foundation, and the W.K. Kellogg Foundation, these organizations are working with some of the country’s biggest health care players, as well as with a variety of community development groups and other stakeholders, to build trust, grow capacity, and expand the idea of what it means to invest in the health of a community.
Seeing the Big Picture—and Acting on It
“This isn’t just about one affordable housing deal,” says Robin Hacke, executive director of the Center for Community Investment (CCI). “We want them to be able to come into the system with their eyes open, thinking about the pipeline of transactions, and thinking about the enabling environment that’s necessary to move the pipeline.”
Hacke’s describing the goals of one of the organization’s key programs, Accelerating Investments for Healthy Communities (AIHC), which is designed to increase health system investments in upstream determinants of health, with a particular emphasis on affordable housing. Hacke and her staff are engaged in an extremely hands-on process to help hospitals better understand the communities they’re working in and their own potential contributions, and then translate that understanding into a sense of confidence to act on affordable housing investments.
AIHC, which began in January 2018 with a group of executives from eight large health care systems, asked participants to stretch from the beginning: “We started by saying they had to nominate a cross-disciplinary team” in order to be able to take part in the initiative, says Hacke.
She and her staff urged the leaders to think beyond the usual suspects and bring in hospital staff with other expertise: employees in finance, for example, or facility management. After all, a hospital has far more resources to potentially invest in a region than simply community benefit dollars; it may have an endowment, a capital budget, mandated or voluntary cash reserves, or significant real estate, all of which could potentially be put to work. And many other departments—like the one in charge of managing Medicaid benefits—stand to gain from improved community health.
Over the course of five months, the diverse groups systematically examined their hospitals’ community investment initiatives and available resources in the context of the actual communities and their needs.
That was the first phase of Accelerating Investments for Healthy Communities, and it was very useful, says Hacke. “The key takeaway for us in phase one was that people were using grant resources in ways that were spending rather than financing.” If those dollars had earned a return, they could have gone much further.

Arrowhead Grove in San Bernardino, California. Photo courtesy of Arrowhead Grove
But nonetheless, even this early phase had impressive results. In San Bernardino, California, for example, Dignity Health reached out to the state’s Strategic Growth Council to discuss an affordable housing project, and the council wound up committing $20 million to the initiative. And in Toledo, Ohio, another participant, the health care system ProMedica, decided to partner with the Local Initiatives Support Corporation (LISC), providing the neighborhood development organization with $20 million in grant funding and $10 million for a loan fund.
The initiative’s second phase began in January with six health care systems. This portion of the program will be much more intensive, guiding participants to examine what it will take to close affordable housing deals: the range of players involved, the many sources of money required, and the changes to their own operating procedures or to the larger policy framework that might be needed for it all to come together. Lasting for two years, the second phase will include learning labs, monthly coaching calls, and local strategy sessions to help participants with specific challenges.
For this second phase, the health care systems have been asked to put together teams even more diverse than in the first phase and including community stakeholders from outside the hospital as well: representatives of neighborhood groups, faith-based organizations, or affordable housing developers.. “Our belief is, if you align stakeholders, there’ll be more for everybody,” says Hacke. “You’re getting the benefit of each other’s wisdom.”
The health care system Bon Secours Mercy Health has staff participating from both its Baltimore and Cincinnati locations. Dr. Samuel Ross, the institution’s chief community health officer, says his hospital joined the initiative in order to better understand all the parts that will have to come together to advance affordable housing in the system’s two communities.
Bon Secours (the system merged with Mercy Health in September) has been involved in CCI’s program since the beginning, and Ross says he’s appreciated the push to think more broadly about potential partners and allies. The institution has created some affordable housing, but Ross says most of it was done through low income housing tax credits, which could be threatened due to the 2017 tax cut. “Robin’s challenge to us is, ‘OK, guys—can you be open to evaluating other ways to expand affordable housing?’”
In response, Ross and his team are learning how to do that. “If affordable housing is embraced as a game changer and a transformational initiative, what we’ve all struggled with is the ‘how,’” says Ross. “One of the benefits of CCI and especially this two-year initiative is it takes us a long way to understanding the nuances of the how—the depth and breadth of expertise, commitments, and sheer willpower that’s going to be required in order for it to be accomplished.”
Helping Nonprofits Up Their Game
On the other side of the equation is the Nonprofit Finance Fund (NFF). Just as CCI helps health care systems expand their thinking about community investments and connect with potential partners, NFF works directly with community-based organizations to help them work with healthcare organizations as equals and better absorb the capital that hospitals are considering utilizing.
NFF has been focused on partnerships between nonprofit groups and health care systems for several years, and it launched a new project, the Healthy Outcomes Initiative, in late 2016. The initiative aimed to address one of the main quandaries in the field: a health care institution’s money is worthless if community development groups aren’t in a position to absorb that funding and put it to good use. To some degree, it’s an issue of underdeveloped skills and capacity on the part of the organizations. But it’s also a matter of habit.
“In the social sector in general, services aren’t typically funded based on full costs,” explains Nima Krodel, NFF’s vice president, who led the initiative. The result is a partnership model between health care institutions and social service groups that’s not particularly equal or durable. “There are a lot of pilots, demonstrations, and smaller-scale experiments about how community-based organizations can partner” with hospitals, says Krodel, “but on a large scale, getting to sustainable, equitable, contractual relationships is further off and where we need to head towards.”
To begin creating those relationships, NFF staff spent two years working directly with community organizations through convenings, workshops, and cross-sector dialogues with hospital executives. NFF heard about their experiences of partnering with nonprofit groups. But perhaps more powerfully, NFF provided the organizations with intensive, one-on-one coaching to help them develop robust cost analyses that translated into sustainable pricing and build their capacity in order to better utilize funding coming in.Among other things, says Krodel, the goal was to have “clear and equitable relationships; that’s the holy grail. To do that, you’d develop contracts”—as opposed to receiving one-time grants—“price them appropriately, and develop new ways of funding and financing.”
One of the beneficiaries of NFF’s efforts was the Pittsburgh-based Community Human Services (CHS). CHS was negotiating a program with the University of Pittsburgh Medical Center in which the hospital would pay the community group for housing some of the institution’s highest users, subsequently reducing its medical costs. Through a partnership with the Corporation for Supportive Housing, NFF helped CHS structure the deal.
Jeremy Carter, CHS’s chief housing officer, says the consultations were invaluable. “We’d never done this before. The biggest impact from NFF was getting us to a better place on the true costs of the program. That’s something that we have struggled to really identify,” says Carter. NFF helped his organization establish a solid indirect rate for the organization and a responsible budget that didn’t undersell their services. “They said, ‘Advocate for yourselves as a nonprofit!’”
And NFF, together with the Corporation for Supportive Housing, helped CHS add an innovative pricing structure into the contract that rewards CHS with a bonus for every patient who remains in housing for over 10 months and a share of the savings when those patients’ medical costs go down. “There isn’t [another] model like this in the country right now,” says Carter.
The Healthy Outcomes Initiative wrapped up in mid-2018, and now NFF is launching a follow-up program called Advancing Resilience and Community Health (ARCH). Rather than focusing on individual organizations, ARCH will work with existing networks of community-based groups, together with the providers or payers that they’re aiming to partner with. Details of the program are still being hammered out, but it is slated to include three networks that NFF will work with over the course of 30 months, with an ultimate goal of establishing standardized models that can be replicated by networks elsewhere.
“There’s no shortage of pilots and waivers to test things out. But unless those move to the next stage and have broader replication, all you’re really doing is having these little experiments,” says Bill Pinakiewicz, NFF’s chief strategic innovation officer. “These are groups looking to build new payment models and contracts together. We’d like to help build that road map and share stories of what it looks like.”
Thinking More Broadly About What Spending and Hiring Can Do
In early 2017, representatives of 10 health systems came together to share their knowledge and questions about how to effectively address some of the upstream factors that were keeping their patients sick. Two years later, that group has swelled to 42, and it’s still growing.
The Healthcare Anchor Network (HAN), unlike CCI or NFF, isn’t primarily concerned with strengthening interactions between community development organizations and hospitals or insurers. That might be on the table, but above all, HAN is focused on health care groups learning from one another to best leverage their assets—all of their assets—to boost the health of their communities.
“The core of what we’re doing is three areas: hiring, purchasing, and investing,” says Dave Zuckerman, director for healthcare engagement at HAN, which is supported by the Democracy Collaborative. So discussions might center on how to leverage new funds to make grants or loans to community groups. But they might also address how a hospital can boost an area’s economic health by more strategically hiring from the community itself and increasing professional development opportunities. Or whether it can do a better job of keeping some of its procurement local.
“We’re very focused on human resources, the supply chain, and core businesses practices that could more powerfully address the issues of poverty and other disparities,” says Zuckerman. “These are systemic problems, and we’re not going to address them by writing a few more checks. It’s about aligning and leveraging resources differently.”
Health care systems pay to be part of HAN, and a big part of the group’s appeal is the peer-to-peer dialogue that occurs there. It’s not unusual, says Zuckerman, for a health care executive to invite a colleague from another institution to visit and share their experience with senior leaders. It’s also common for staff from across a hospital to be invited to participate—including folks in charge of, say, facilities or government relations—so that they too can become champions of impact spending.
With an eye toward making dollars and efforts go further, HAN members are also beginning to advocate more broadly for policy priorities. On Feb. 28, the group will advocate on Capitol Hill in an effort to educate members of Congress about the relationship between housing and health, and perhaps nudge them to support beneficial policies.
One of the speakers in Washington that day will be Thea James, vice president of mission at Boston Medical Center. She and her colleagues at Boston Medical are wholly on board with efforts to promote Boston’s health by focusing on upstream factors. They’ve helped to organize a sub-network among HAN member hospitals in New England and are part of a committee within Boston Medical designed to disseminate knowledge among staff.
Thanks to ideas discussed among the full group, Boston Medical has begun examining how many of its vendors are minorities, women, or people with disabilities. “Those things impact the community and contribute to economic development there,” says James. “It’s good for us to see how other [healthcare systems] do it so we’re not reinventing the wheel.”
Moving Forward With a Big Idea
Enterprise Community Partners has long helped finance complex affordable housing deals around the country, so it’s unsurprising that it has become a major player in addressing upstream determinants of health. Enterprise is collaborating with the Denver Housing Authority, for example, to help find sustainable ways to partner with the health care sector. In Detroit, the organization is part of a public-private partnership led by Sinai-Grace Hospital to explore potential neighborhood revitalization projects.
But in its work in the burgeoning field, the company has identified some limitations.
“In other [Western] countries, many of these classes of investment are seen as public goods, financed through different tax structures,” says Brian Rahmer, vice president of health and housing at Enterprise Community Partners. That is, because so many people and institutions benefit from a healthy population, investments in things like affordable housing, early childhood education, and a social safety net are paid for by taxes in most developed countries.
In this country, the private sector may be hesitant to fund programs that improve health because they might receive only partial returns. For instance, an insurance company that finances the construction of an affordable multifamily building won’t recoup its full investment if only some of the residents are covered by its policies.
To address that, Enterprise has begun thinking about a new model. In August 2018, Health Affairs—a peer-reviewed journal of health policy thought and research—featured an article by Len Nichols and Lauren Taylor describing how health care institutions, working with community development groups, could provide some of those public goods and still earn a return on their investment.
Nichols and Taylor suggest that a “trusted broker”—a financially neutral organization like a nonprofit or foundation—convene all of the potential players in such a deal. The broker would transparently select an intervention, project its return on investment, assign a portion of the cost to each of the major stakeholders in proportion to their potential gains, and implement the intervention. So a hospital system that would gain the most for keeping someone out of the emergency room would pay a greater share for an affordable housing project than a homelessness service provider whose savings would be less.
The role of the broker could be filled by any skilled organization, including Enterprise. And an effective model doesn’t have to look exactly like Nichols and Taylor’s. “Boiled down, we want to be able to create an investment portfolio at the regional or local level allowing multiple stakeholders to have a very easy pathway to drive their money, with a floor in terms of the return,” says Rahmer.

Kensington Gardens, a 41-unit apartment building in the East Bay area, was directly impacted by the Housing for Health Fund. Kaiser Permanente is partnering with Enterprise and the East Bay Asian Local Development Corporation to ensure the property gets needed upgrades and is preserved as affordable housing. Photo courtesy of the East Bay Asian Local Development Corporation
And that’s happening now. In January, Enterprise announced several new initiatives. Partnering with Kaiser Permanente, the organization has set up an equity fund that will grow to as much as $85 million through matched investments for the greater Bay Area, and another $100 million loan fund covering regions across the U.S. where Kaiser operates. And over the next five years, Enterprise is committing $250 million to, among other things, bring together “capital from health care organizations, institutional investors, and social impact funds” to develop and preserve affordable homes.
These funds are intentionally set up to drive health outcomes in the communities where they operate. Enterprise is guaranteeing a 4 to 5 percent return on investment to Kaiser; that’s less than what it could earn on the private market, but for a mission-driven organization, it’s significant.
The new initiatives aren’t the final answer, Rahmer acknowledges. “Are we there yet? No. But we’re creating these pathways now to allow solutions to come to fruition,” he says. “The resources currently in play are not having the impact that we want them to make. Capital is only good if it does something. So what does it do? That’s part of the equation that we’re trying to correct.”
After all, in this country, government isn’t able or willing to spend big on the upstream factors that significantly impact people’s health. In response, Enterprise and many other groups are stepping in to find a new source of revenue that might do the trick. The big question is whether their efforts will be able to wring enough funding from the giant healthcare industry—and whether hospitals and insurers will find the work worth their own while.
Editor’s Note: This article has been updated to clarify information about an equity fund set up by Enterprise and Kaiser Permanente.
Comments