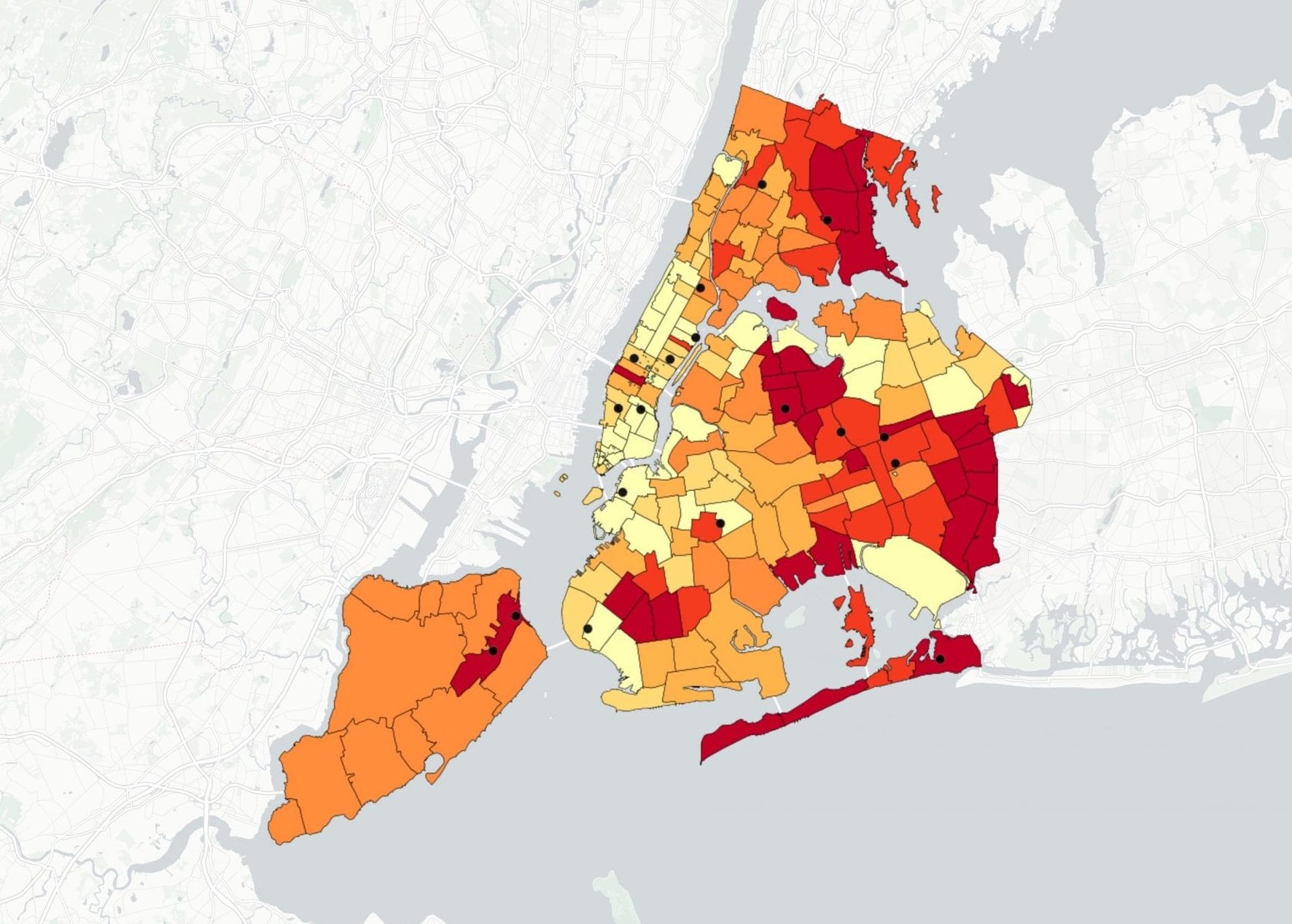
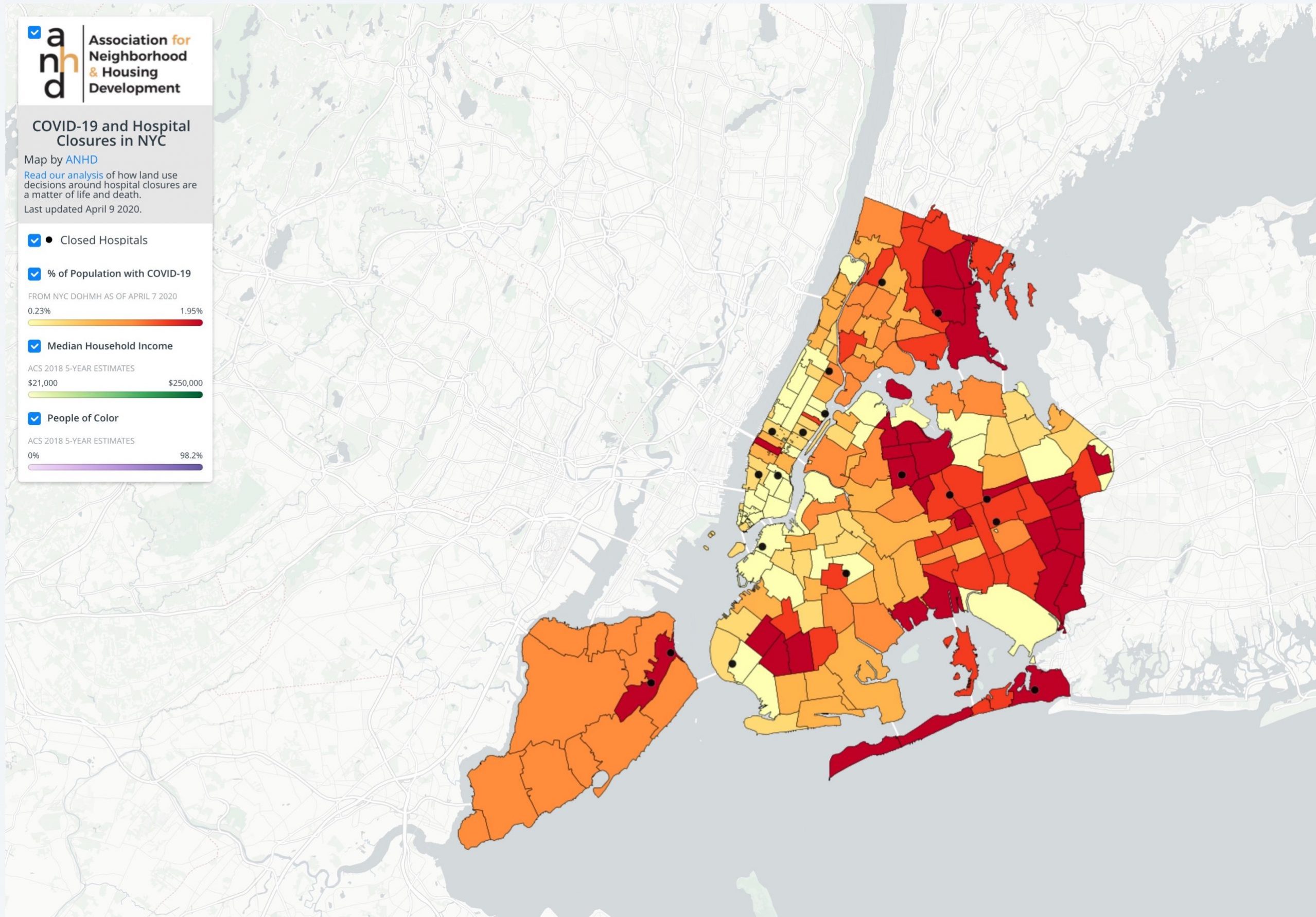
A map by the Association for Neighborhood and Housing Development that highlights hospital closures in New York City. Click on the map for a deeper data dive. Courtesy of the Association for Neighborhood & Housing Development
New York City remains the epicenter of the global COVID-19 pandemic, but its effects are being felt differently across neighborhoods. As the Association for Neighborhood and Housing Development’s previous analysis shows, this virus is hitting low-income communities of color the hardest. The neighborhoods with the highest range of positive COVID-19 cases in the city are home to communities of color whose residents are disproportionately employed in frontline service occupations and face among the highest rates of rent burden and overcrowding. These communities—the epicenters of the epicenter—are home to the largely invisible workforce that is keeping New York City running in this moment of crisis, and they are the ones who are bearing the brunt of its impacts. Recent data released by the city’s Department of Health shows that Black and Latinx New Yorkers are dying at twice the rate of whites—making clear that this pandemic is not only a public health crisis, but a crisis of racial and economic justice as well.
Among the host of historic inequities behind the disparate impact of COVID-19, one is particularly striking: the string of hospital closures that took place in these communities over the past few decades. At least 18 hospitals have closed all of their inpatient services in New York City since 1998—leading to the loss of thousands of hospital beds—with two-thirds of those closures occurring in the outer boroughs. A look at the data shows that the majority of these outer borough hospital closures fell in lower-income communities of color that bear the brunt of the coronavirus crisis today. These community hospitals catered to neighborhood residents, many of whom lack private insurance; the mass closure and downsizing to outpatient services means less access to necessary health services, especially in a time of crisis. Households without health insurance have few options if they get sick, other than visiting the remaining public hospitals, adding to the likelihood of exposure to coronavirus and the further straining of the health care system.
While community hospitals were being closed in low-income communities of color, hospitals in wealthier sections of the city were being converted into luxury residential buildings, further depleting the city’s overall supply of hospital beds. Of the 18 hospitals that closed in the last two decades, over 40 percent have been replaced by residential developments, most of them with rents or sales prices that are astronomically out of reach for the average New Yorker. At the site of St. Vincent’s Hospital in Manhattan, where countless poor New Yorkers received care during the AIDS crisis, now stands Greenwich Lane, a luxury condo building. Long Island College Hospital in Brooklyn, a community medical facility known as America’s first teaching hospital, was replaced by 5 River Park where a studio apartment was recently sold for $1.15 million.
In Queens, the epicenter of the COVID-19 crisis, the closures of St. John’s Hospital, Parkway Hospital, and Mary Immaculate Hospital have led to massive overburdening of nearby medical facilities. The neighborhoods where these hospitals were once located in have some of the highest rates of COVID cases in the city. The former site of St. John’s Hospital is located just blocks from Elmhurst Hospital—the same hospital that has seen among the most COVID-19-related deaths in the country. What stands in its place now is Queens Pointe, a market-rate apartment building. The former site of Mary Immaculate Hospital in Jamaica—another COVID-19 hotspot—was transformed into a residential development in 2009. Nearby Parkway Hospital, which once served low-income Queens residents, was also torn down to make room for a residential building in 2008.
As these hospitals continued to serve poor and uninsured New Yorkers, financial restructuring and an inability to pay their bills contributed to a spate of closures in the late 2000s. The deprioritization of hospital infrastructure and subsequent development of residential—particularly luxury residential buildings—on these former hospital sites is the direct result of the city’s land use decisions. The Bloomberg era saw a pattern of high profile rezonings of both public and private land to facilitate luxury residential development, with few if any public benefits secured in exchange for the enormous value these conversions provided to private real estate developers. The prioritization of profit over community need has left a long-lasting legacy across New York, and communities of color have continued to face the brunt of it through displacement, housing instability, job loss, and health disparities. Communities and advocates have long said that these land use decisions have life and death consequences; we as a city are now forced to reckon with the consequences of those decisions in this moment.
The story of hospital closures follows an all-too-familiar pattern of disinvestment and a lack of resources in low-income communities of color throughout the city, combined with a focus on luxury housing development that doesn’t come close to serving New Yorkers most in need. While the details may vary in terms of which private and governmental entities are driving the decision making, the general story is the same: capital investment and land use decisions have led to an inequitable distribution of resources and opportunity across our city. Whether it’s access to critical infrastructure, good-paying jobs, or truly affordable housing free from the risk of displacement and overcrowding, the failures of our planning processes have exacerbated inequality within New York City in a way that is playing out in life or death terms today.
The Association for Neighborhood and Housing Development (ANHD) has called for immediate policy solutions to the COVID crisis—including rent relief, hazard pay, and increased worker protections regardless of immigration status—to support frontline communities in this vital moment. But as we begin to imagine our future in this new COVID reality, we must acknowledge the failures that helped bring us here and commit to a comprehensive planning approach that centers equity and uses a full range of land use, budgeting, and policy tools toward the central goal of reducing the structural inequities that this crisis has laid all too bare.
This post originally appeared on ANHD’s blog.



I have mixed feelings about this piece. I wholeheartedly agree that land-use decisions have implications far beyond housing and that is certainly true in NYC. And, the inequities we are seeing in this current crisis are heartbreaking. However, I think this article makes a critical error in placing the blame far too quickly and easily on developers for the replacement of hospitals with market-rate housing. The closure of hospitals is a financial decision that largely stems from our failed healthcare policies in the U.S., amplified in New York by the increasing inequalities there. Running a healthcare system as it is designed in America is extraordinarily expensive (our per capita health expenditures are highest among OECD nations), which inherently prices out those without insurance and subsequently those facilities that serve people without coverage. Yes, our land use decisions matter immensely–I would never argue against that–but the issue of healthcare deserts isn’t a land use problem, but a healthcare policy one. If the sites of those shuttered hospitals had been zoned only for hospital use, I can all but guarantee they would still be vacant today.
1. This is part of a national trend; the number of American hospital beds has gone down by over 1/3 since 1975, despite an expanding population. https://www.statista.com/statistics/185860/number-of-all-hospital-beds-in-the-us-since-2001/ There’s a really good reason why hospitals everywhere were closed in recent decades. Decades ago, it was normal for a person in good health to be hospitalized for all kinds of reasons- for example, childbirth. Today, people aren’t hospitalized as frequently- so Americans don’t need as many hospital beds as they did in 1963.
2. I don’t see why its so terrible that hospitals are being replaced by housing for human beings. Would the author prefer that they be replaced by vacant lots?